What Is Cubital Tunnel Syndrome?
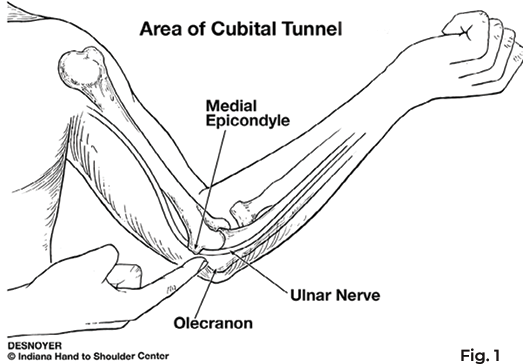
The cubital tunnel is a passageway between the bony prominence of the inside elbow (medial epicondyle) and the tip of the elbow (olecranon process). Through this passageway travels the ulnar nerve as it crosses from the arm to the forearm behind the flexion-extension axis of the elbow (Fig. 1). When the ulnar nerve is injured or compressed, it causes cubital tunnel syndrome.
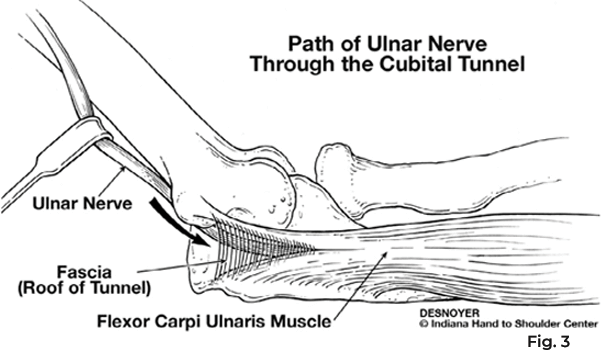
To keep the nerve in its place with motion of the elbow, the tunnel is covered with tissue called fascia. The ulnar nerve exits the tunnel and passes between the two muscle origins of the major wrist flexor muscle, the Flexor carpi ulnaris muscle.
What Are the Signs and Symptoms?
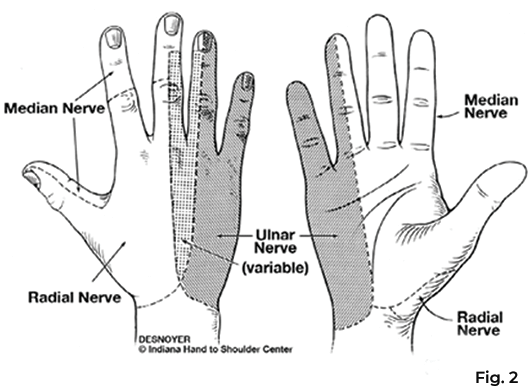
The ulnar nerve provides sensation to the little finger and half of the ring finger. It supplies several muscles in the forearm, but most importantly, it controls many of the small muscles in the hand responsible for coordinating finger motion and pinch.
Patients with cubital tunnel syndrome commonly exhibit intermittent numbness or tingling in the ring and little fingers of the affected extremity, and eventually weakness and loss of fine manipulative hand coordination. These symptoms may occur with prolonged elbow flexion or putting resting pressure against the elbow where the nerve passes.
There may be an associated aching discomfort along the inner forearm or elbow. If microcirculation of the nerve is compromised by prolonged traction or compression, there can be permanent loss of sensation in the ring and little fingers, and eventually, there is a loss of pinch and grip strength.
Tapping over the ulnar nerve at the cubital tunnel can produce “electric shocks” or tingling (Tinel’s sign) radiating into the ring and little fingers. Bending the elbow may reproduce the aching discomfort about the elbow and forearm or the tingling in the fingers. There may be difficulty crossing the middle finger over the index finger.
Severe cases will reveal loss of muscle bulk, or wasting, over the little finger aspect of the palm and along the back of the first web space between the thumb and index finger.
Other conditions resembling cubital tunnel syndrome include compression of the nerves in the neck and shoulder area or compression of the ulnar nerve at the wrist. These conditions can often be excluded by physical examination. However, it may be necessary to obtain special X-rays, vascular tests, or nerve testing to help with the diagnosis.
What Are the Causes?
There are many ways in which the ulnar nerve can be injured or compressed in the cubital tunnel:
- Either a severe, direct impact to the inner aspect of the elbow or chronic pressure to this area (such as supporting the arm by resting on the elbow) may produce swelling and inflammation within the cubital tunnel irritating the ulnar nerve. Over time, this may lead to scar tissue formation in and about the ulnar nerve, compromising its microcirculation.
- Either a severe, direct impact to the inner aspect of the elbow or chronic pressure to this area (such as supporting the arm by resting on the elbow) may produce swelling and inflammation within the cubital tunnel irritating the ulnar nerve. Over time, this may lead to scar tissue formation in and about the ulnar nerve, compromising its microcirculation.
- The fascial covering of the cubital tunnel may lose its ability to stabilize the ulnar nerve with elbow motion. The nerve then becomes exposed to repetitive trauma as it slides in and out of its normal position.
- Injury to the elbow joint bones may produce changes in the alignment or carrying angle of the joint. This may place tension on the ulnar nerve or narrow the size of the cubital tunnel.
- As the floor of the cubital tunnel is formed by the elbow joint, arthritis may produce swelling or enlargement of the joint, which in turn narrows the cubital tunnel compressing the ulnar nerve.
- Masses and space-occupying lesions such as ganglion cysts or anomalous muscle tissue can compromise the space available for the ulnar nerve within the cubital tunnel.
How Is Cubital Tunnel Syndrome Treated?
In the early stages, cubital tunnel syndrome symptoms may be alleviated by avoiding activities requiring prolonged or repetitive elbow flexion or resting against the elbow. To prevent elbow flexion, particularly at night, it may be necessary to use a long-arm splint. An elbow pad worn during the day can be beneficial in protecting the cubital tunnel from direct pressure. An oral anti-inflammatory can help alleviate symptoms.
Surgery may be indicated when cubital tunnel syndrome is severe or fails to improve with conservative management. The goal of surgery is to relieve the compression of the ulnar nerve within the cubital tunnel. The simplest approach involves dividing the tissue overlying the ulnar nerve at the elbow.
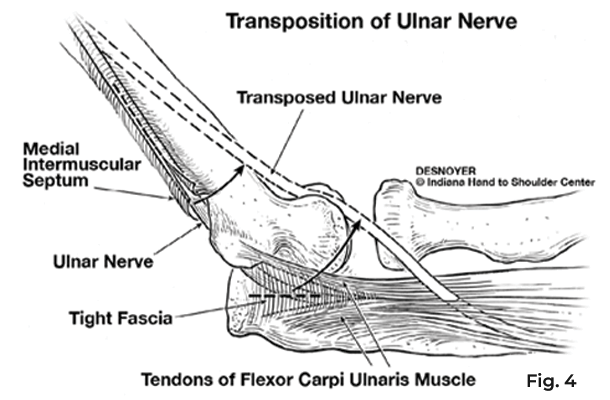
If the ulnar nerve is more severely affected, it may be necessary to move the nerve out of the cubital tunnel to the front of the elbow. (Fig. 4)
The nerve can be placed in the fatty layer of soft tissue within the forearm muscles. Following surgery, the arm is immobilized in a long-arm bulky dressing with a plaster splint. (Fig. 5)
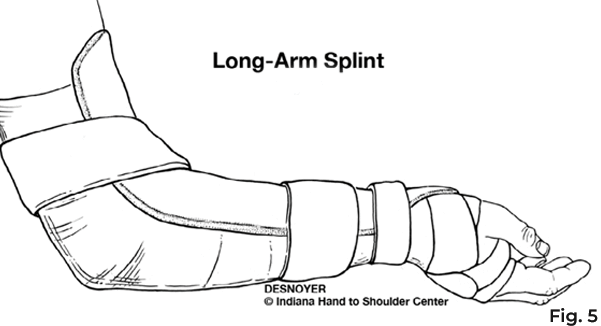
Elevation and finger motion is important to prevent swelling during the post-operative period. This dressing is usually removed two to three weeks after surgery to permit suture or staple removal and begin range-of-motion exercises.
Additional elbow immobilization may be required between exercises for up to three additional weeks after surgery. Strengthening of the extremity can begin four to eight weeks after surgery, depending upon the procedure performed.
What About Recovery?
Recovery from cubital tunnel syndrome surgery requires two to three months before resuming the extremity’s unrestricted use. Several months may be needed before the maximum benefits of surgery are achieved.
Even with surgery, cases with severe loss of sensation or muscle wasting may not recover completely, although pain relief can usually be attained even in severe cases. With proper diagnosis and appropriate treatment, the progression of this condition can be prevented.
No part of this work may be reproduced without written permission from the Indiana Hand to Shoulder Center.
Disclaimer: The materials on this website have been prepared for informational purposes only and do not constitute advice. You should not act or rely upon any medical information on this website without a physician’s advice. The information contained within this website is not intended to serve as a substitution for a thorough examination from a qualified healthcare provider. The display of this information is not intended to create a health care provider-patient relationship between the Indiana Hand to Shoulder Center and you.


Cubital Tunnel Syndrome Patient Handout